5. Referral to specialist centres
Complex open lower limb fractures require a multidisciplinary approach involving plastic and orthopaedic surgeons with sufficient experience to manage such injuries. Usually, the initial assessment on the scene is carried out by the ambulance service and patients are appropriately triaged directly to a trauma centre that has the necessary expertise for the degree of injury. However, when patients present to a hospital in which such a team is unavailable, prompt referral and transfer to the nearest specialist centre is essential.
In addition, there are specific features of open tibial fractures that warrant referral to specialist centres and clinicians should be alert to these. These features are based on certain patterns of fractures and soft tissue injuries.
5.1. Fracture patterns
- Transverse or oblique tibial fractures with fractures of the fibula at a similar level.
- Segmental tibial fractures.
- Fractures with bone loss either at the time of injury or following debridement.
- Fractures of the tibia with comminution or butterfly fragments with concomitant fibular fracture at a similar level.
5.2. Soft tissue injury patterns
- Degloving (avulsion type injury, where the skin and/or soft tissues are torn from their neighbouring tissues, culminating in disruption of blood supply to the affected tissues).
- Loss of skin such that tension-free wound closure is not possible.
- Injury to one or more of the major arteries of the lower limb.
- Injury to the muscles that requires excision of devitalised muscle.
6. Compartment syndrome
The lower limb is divided into four discrete compartments by the investing deep fascia: the anterior, lateral, superficial and deep posterior compartments (Figure 8.3). An increase in pressure within these fixed osseofascial compartments can compromise tissue perfusion of the lower limb, resulting in myoneural necrosis and ultimately loss of limb function. Post-ischaemic reperfusion injury and direct crush injuries of the limb are frequently associated with an increase in intra-compartmental pressure. This is a surgical emergency which needs to be diagnosed and treated immediately.
Although compartment syndrome occurs more commonly after closed leg injuries, it can also occur following open tibial fractures (reported as 2–9%) (Park et al., 2009). A high index of suspicion should be maintained for high-energy fractures and unconscious patients.
The principle signs of compartment syndrome include marked pain out of proportion to the injury, tenderness on palpation of the compartment, pain on passive movement of the muscles affected, paraesthesia and paralysis of the limb. Absent pulses are a late sign and are not specific to compartment syndrome.
Therefore, their presence should not exclude a diagnosis of compartment syndrome. Pulses are characteristically lost in prolonged compartment syndrome where muscle necrosis has usually occurred, but should also alert the surgeon to the possibility of a vascular injury.
A definitive diagnosis of compartment syndrome can only be made upon measurement of compartment pressures. It is imperative that every effort is made to make an accurate diagnosis because inappropriate fasciotomies can be linked to significant morbidity.
In any case of suspected compartment syndrome, compartment pressures should be estimated using a specific transducer such as the Stryker intra-compartmental pressure monitor, ideally from all four compartments. An increase from normal tissue pressure (2–7 mmHg) to 30 mmHg indicates a high likelihood of compartment syndrome, and pressures of 35–40 mmHg are an absolute indication for decompression.
A more accurate measure of compartment pressure is the differential pressure (diastolic pressure minus compartment pressure). A differential pressure of <30 mmHg is an indication for fasciotomy or decompression (McQueen & Court-Brown, 1996).
6.1. Treatment of compartment syndrome
Diagnosis and early intervention are of the utmost importance in the management of compartment syndrome. Tissue injury becomes irreversible within a couple of hours, with resultant muscle and nerve loss. The definitive management in such a circumstance is four-compartment fasciotomy of the lower limb to decompress the compartments (Figure 8.3).
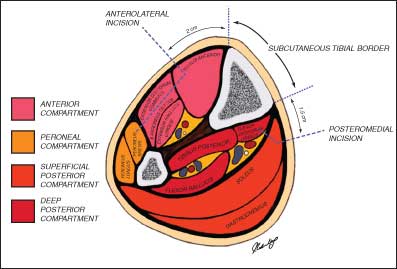
Figure 8.3. – Cross-sectional anatomy of lower limb and approach to four-compartment fasciotomy in compartment syndrome. – Source: Rebecca Nicholas.
The subcutaneous borders of the tibia are identified and vertical skin incisions are placed at 15 mm from the medial border and 20 mm from the lateral border. The careful placement of these incisions is essential in order to preserve perforators which may be important for subsequent soft tissue reconstruction (see below). The superficial posterior compartment is decompressed through the medial incision. The fascia overlying the posterior tibial neurovascular bundle at the ankle is incised upward, detaching the soleus muscle from its origin from the tibia and subsequently decompressing the deep posterior compartment. The lateral incision decompresses the anterior compartment; from here, the lateral intramuscular septum is divided, releasing the peroneal compartment.

