1. Introduction
Arm contouring is one of the most emerging topic in body contouring. In this chapter conventional liposuction with laser assisted liposuction (LAL) is proposed to yield satisfactory results in selected group of patients. Classification systems are helpful to decide for proper patient selection for this technique. It includes assessment of fat excess, skin excess, and location of the deformity (proximal, entire arm, arm and chest). Patients with minimal to extensive fat deposits plus minimal to moderate skin laxity are the best candidates for this approach.
When properly performed, with realistic expectations, liposuction and LAL combination is considerably a procedure of choice for arm contouring in these selected cases. The contraction of arm skin is considerably consistent. Our approach, except in the most extreme cases, is to initially recommend liposuction and possibly even a second liposuction prior to recommending brachioplasty. An esthetically pleasant result can be obtained even in massive arms with good skin tone. Massive arms with poor skin tone, however, may not.
This chapter reviews the relevant literature in arm contouring including surgical and minimal invasive procedures used to esthetically improve the arm. Patient selection and preoperative planning are discussed in detail. A thorough description for patient positioning and anesthesia options are studied. The technique of the liposuction is widely described including specific regional contour goals with artistic attention to enhance the contour. Refinement regarding skin tightening and skin surface smoothness are also discussed.
1.1 Overview
-
Selection of Candidates, Preoperative Planning, Preoperative Photo documentation
-
Patient Positioning, Anesthesia Options
-
Infusion, Traditional Liposuction, Selection of Liposuction Cannulas, PAL (Power-Assisted Liposuction), Water-Jet asisted liposuction
-
Toning and Smoothing of the skin
-
Art of Arm Contouring (regional boundary goals, and how to achieve them)
-
Postoperative Care (compression garments, activity restrictions)
-
Prevention of Complication and Complication Management
2. Selection of candidates, preoperative planning, preoperative photo documentation
2.1 Selection of candidates
-
One of the most crucial steps in body and arm shaping operations is the selection of candidates. In order to have the best result after a liposuction procedure, patient selection has to be done very carefully. Correct selection of the patient is one of the most important determinants in obtaining the desired result after the liposuction procedure. Thus detailed physical examination during the assessment of a patient has a great importance.
-
There is not only one reason behind the upper arm deformities. It may occur due to the accumulation of an excess fatty tissue,which is called lipodystrophy, or in some cases skin laxity might be the only reason for upper arm deformities. However, coexistence of both causes may result in upper arm deformities.
-
Patients who will be selected for a liposuction procedure, should have a good skin elasticity with little skin laxity and there should be no or limited excess skin. In patients with excessive skin laxity, it is not possible to reach the ideal result solely with liposuction. Skin resection might be required in patients who have severe skin laxity or extreme excess skin.
-
Various algorithms and classifications have been described to decide the surgical procedure that is going to be applied [1, 2, 3]. In 1998, Teimourian and Malekzadeth have defined the first classification system by diving the patients into 4 groups. Patients who have mild or moderate fatty tissue and mild skin laxity are defined as group1 and liposuction procedure alone is preferred option.
-
However, depending on the degree of fatty tissue a combination of liposuction or only resection is recommended for patients in other groups with more skin laxity [1]. Applelt et al. expanded the classification system to include the location of excess skin and severe deformities involving the arm and lateral chest wall, were added into the indications for brachioplasty [2, 4]. Although, El Khatib’s classification of brachial ptosis is similar to these classifications, it includes the measurement of the amount of skin ptosis under the brachial sulcus.
2.2 Preoperative planning
-
In body shaping procedures, preoperative surgical marking during preoperative planning has a great importance for an optimum result. Preoperative surgical marking has to be done with detailed physical exam while the asymmetries are also need to be addressed as well. In the presence of assymetry, patient should be informed regarding the postoperative result. As a result of physical exam, the concavity and convexity should be determined and marked.
-
These markings will be guiding the surgeon during the surgery and will also decrease the risk of contour deformities by applying the liposuction to the appropriate areas as needed. Preoperative marking should be done in standing position. Patient’s shoulders must be placed in 90 degrees of abduction and elbows should be positioned at 90 degrees of flexion. This position will help to assess the skin laxity, skin excess and the degree of ptosis. Surgeon will able to evaluate the contour deformities while the patient’s arm are in full extension. Preoperative surgical markings should be checked one more time after the patient is placed on the operation table.
3. Patient positioning, anesthesia options
3.1 Patient positioning
-
Patient should be placed in supine position on the operation table. After the patient is taken to the surgery room, the preoperative surgical marking should be checked one more time. Arms should be freely positioned to facilitate arm movement during liposuction procedure. If circumferential liposuction is planned, the arm should be considered into 3 units as medial, lateral and posterior and liposuction needs to be performed in a sequential order.
3.2 Anesthesia options
-
The type of anesthesia can be decided based on the preference of the patient and the surgeon, the amount of fat and the necessity of ancillary surgical procedures to be applied. If it is a limited volume liposuction and no additional surgical procedures is planned then, local and regional anesthesia may be the type of anesthesia chosen. If it is going to be a large volume liposuction and h additional surgical procedures will be added then, general anesthesia may be preferred. The importance of fluid replacement should be kept in mind throughout surgery. And it is crucial especially for mega volume liposuction.
4. Infiltration, traditional liposuction, LAL, PAL, selection of liposuction cannulas
4.1 Infiltration
-
It is of great importance and practice to apply infiltration solution before starting the liposuction procedure. The tumescent technique containing diluted epinephrine and lidocaine, which is frequently used in liposuction practice today, was described by Jeffrey Klein [5]. Reasons and advantages beyond application of infiltration solutions are a few.
-
Epinephrine and lidocaine in the solution have two basic roles: anesthesia and vasoconstriction. Thanks to the vasoconstrictor effect, bleeding during the procedure and bruising in the post-operative period are reduced considerably. For patients whom general anesthesia is not preferred, liposuction can be performed with infiltration thanks to its anesthetic effect.
-
For patients undergoing general anesthesia, intraoperative anesthesia is supported and patient comfort is increased in the post-operative period thanks to this anesthetic effect. It is not an obligation to use lidocaine in the infiltration solution in patients undergoing general anesthesia. However it is generally preferred because of these secondary effects. In order to reduce the risk of toxicity, the amount of lidocaine dosage should not exceed 35 mg/kg [6]. The infiltration solution commonly used today is a mixture of 1 ml of epinephrin (1:1000) and 50 ml of 1% lidocaine for 1 liter of Ringer lactate solution [7].
-
While the ratio of infiltration solution to aspirate volume is approximately 2–3:1 in the tumescent technique, which is one of the most widely used infiltration technique, this ratio is approximately 1:1 in the super wet technique. Application of infiltration solution facilitates the movement of the cannula by providing tissue expansion and decreasing friction forces during the liposuction procedure. The infiltration solution should be evenly distributed to the area of liposuction. Over-infiltration (more than 3:1 ratio) should be avoided as it may cause the surgeon to judge falsely.
4.2 Traditional liposuction
-
In the traditional suction-assisted liposuction (SAL) method, the liposuction process is performed by suctioning the deep fatty tissues with a vacuum driven source providing negative pressure [8, 9]. This method is usually carried out with a device that provides negative pressure with aspiration [10].
-
Ultrasound-assisted liposuction (UAL) is another technique available. UAL may cause a higher rate of seroma formation compared to the traditional (SAL) method. Furthermore, care should be taken to avoid thermal injuries that may occur due to its thermal effect. SAL can be combined with power-assisted liposuction (PAL).
-
A forward moving cannula is used in the power-assisted liposuction (PAL) method. This method can be preferred for patients who have dense soft tissues or secondary cases. One of the greatest advantages is that the surgeon gives less effort and provides suction in more dense areas of fibrous tissue.
-
In laser-assisted liposuction (LAL) method, it is estimated that the laser energy causes the destruction of fatty tissue. One of the most advantage of LAL is its capability for a better skin retraction compared to the traditional method. This is a great value for patients with severe skin laxity. LAL is our preferred method for arm liposuction for this high potential skin contraction feature. Radiofrequency-assisted liposuction (RFAL) method can also be preferred in patients with severe skin laxity to provide a skin contraction and retraction. Care should be taken against thermal injuries that may occur on the skin due to thermal energy during the radiofrequency-assisted liposuction (RFAL) process.
4.3 Selection of liposuction cannulas
-
Cannula options are available in various lengths from 2 mm to 4 mm depending on the amount of fatty tissue in the area to be applied during the liposuction procedure. Cannulas which are small in diameter are used to eliminate surface irregularities and minimize the risk of contour deformity. Care should be taken not to loose the skin tissue during liposuction procedure. Hence, the risk of contour deformity can be minimized by directing the sucking holes apart from the skin surface. A
-
rm shaping procedure with the LAL method, begins with infiltration through two stab incisions near the elbow area. These two stab incisions are desired to be located on the posterior half of the arm and to be at a certain distance from each other to allow cris-cros. Although cris-cros is aimed, it is mainly planned to aspirate regional fat accumulation located along the vertical axis of the arm.
-
In other words, during liposuction, fat aspiration is requested in a single direction, not homogenous and versatile as in abdominal or back region. As the initial step, the process starts as traditional SAL and after the targeted area is aspirated, the laser component is applied alone. According to the tissue elasticity, laser component is applied in certain watts (Orbeam Diode Laser, in a 60-watt laser device, 1000 nm fiber with a 25-watt output and 4500–6500 joules preferred per one arm.).
5. Toning and smoothing of the skin
-
Again, we cannot emphasize enough the importance of selection the appropriate candidates. Liposuction can achieve good results in patients who have mild or moderate fatty tissue, good skin tone, and mild skin laxity.
-
In patients who have severe skin laxity or extreme excess skin, resection based procedures might be applied alone or in combination with liposuction procedure. The biggest downside of resection based surgeries in brachioplasty is the resulted scar tissue in the long axis of the arm. In patients without severe skin laxity and skin excess, energy-based systems might be used to provide a skin contraction of the targeted area. LAL or RFAL methods may be preferred in these patients [11].
-
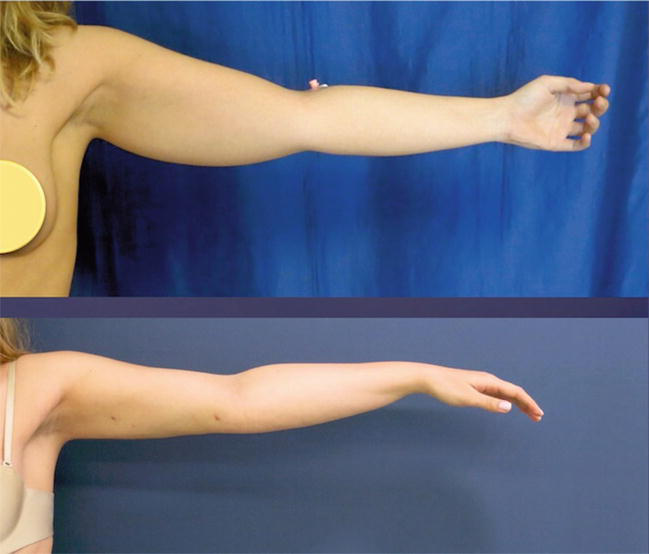
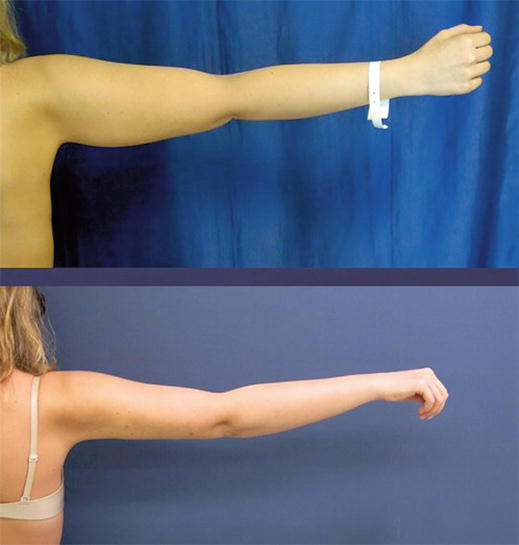
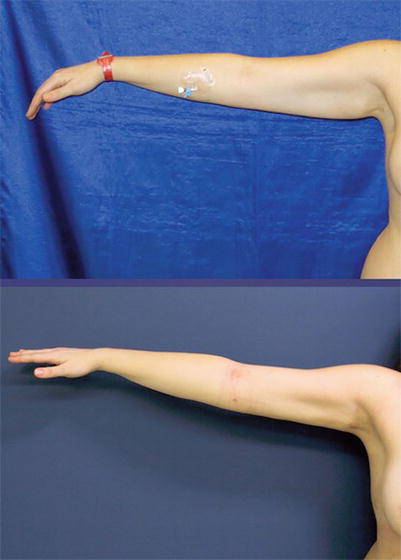
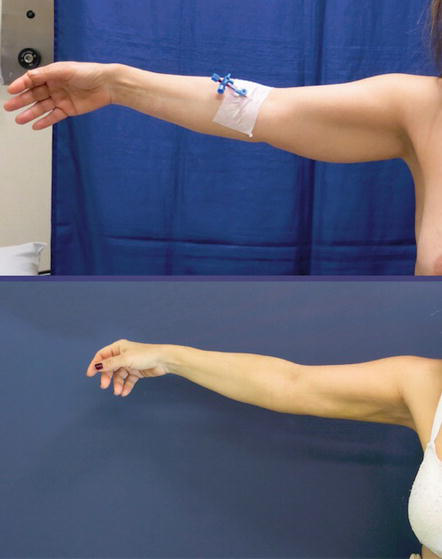
In addition, radiofrequency energy-based skin tightening technique can be combined with the liposuction procedure. It is possible to obtain a more satisfactory result by applying the second LAL session for patients with severe skin laxity or whom desired skin contraction could not be achieved in the first session. It is recommended that a gap of at least 6 months between two sessions would be feasible (Figures 1–8).
-
All patients are undergone only the LAL. No ancillary modalities were applied. We believe patients would benefit from RFAL as well.




6. Art of arm contouring
-
Extreme care should be taken for contour deformities that might occur after liposuction. Considering the convex and concave surfaces of the arm, besides the LAL method, the establishment of concave areas with fat grafting should be considered principally in primary liposuction.
-
Liposuction procedure and fat grafting can be combined to reduce the risk of contour deformity. This will give a more pleasant cosmetic looking and will provide skin quality in selected patients. The fat aspirated from redundant areas of the arm can be used for grafting the fat. This can be of paramount importance specifically while shaping the bicipital groove area with fat grafting [12].
7. Postoperative care, compression garments, activity restrictions
-
Patients should be informed about the post-operative period. In the early phase of post-operative period, patient should be informed about bruising and edema. Especially in the first 2–3 days, the patient should be informed that there might be serious leakage from the incisions. It is completely surgeon’s choice to suture the incision area or not.
-
It is suggested to use compression garments or compression bandages in order to reduce the formation of edema and bruising in the post-operative period. It is believed that this approach accelerates the healing as well. Although applying of compression garments is suggested for an average of 4 weeks, more might be needed depending on individual requirements.
-
Patients are mobilized 3 to 4 hours after the surgery. In the early phase of post-operative period, mobilization should be encouraged but patients should also be informed for avoiding excessive and strenuous physical activity. Patient should be followed up after the first week.
-
If there is not any problem during this one week period, the amount of physical activity can be gradually increased from the first week on. Patients are recommended to perform normal daily activities by avoiding excessive physical activity. Patients who do not have any problems in their follow-up can be allowed for full physical activity, 3–4 weeks after the surgery.
8. Summary
Contouring of the arms is the desired goal of the arm esthetics. Arm lifting is a developing and safe surgery to improve the arm silhouette but scar, all the way along the arm, is one of the most distracting factor for both patients and surgeons.
In this chapter conventional liposuction with laser assisted liposuction (LAL) is proposed to yield satisfactory results in selected group of patients.
Patients with minimal to extensive fat deposits plus minimal to moderate skin laxity are the best candidates for this approach. When properly performed liposuction and LAL combination is considerably a procedure of choice for arm contouring in these selected cases.
The contraction of arm skin is considerably consistent for certain ages and people. Our approach, except in the most extreme cases, is to initially recommend liposuction and possibly even a second liposuction prior to recommending brachioplasty. An esthetically pleasant result can be obtained even in massive arms with good skin tone.
Patient selection and preoperative planning are discussed in detail. A thorough description for patient positioning and anesthesia options are studied. The technique of the liposuction is widely described including specific regional contour goals with artistic attention to enhance the contour. Refinement regarding skin tightening and skin surface smoothness are also discussed.
Arm contouring is a growing field of body contouring and can be practiced with low complication rates and high patient satisfaction. Available classification systems helps to select proper patient group.
Laser assisted fat removal combined with conventional liposuction is an effective combination to provide satisfactory results for selected patients.
Authors
Engin Selamioglu
Department of Plastic Surgery, School of Medicine, Bahcesehir University, Istanbul, Turkey
Ercan Karacaoglu
Department of Plastic Surgery, School of Medicine, Bahcesehir University, Istanbul, Turkey
Attribution
Selamioglu, Engin, Karacaoglu, Ercan. “Enhanced Liposuction for Arms” In Enhanced Liposuction: New Perspectives and Techniques, edited by Diane Duncan. London: IntechOpen, 2021. 10.5772/intechopen.97572
